SlicerIGT is a collection of modules for the 3D Slicer application to support image-guided medical interventions
Surgical device & robot registration
|
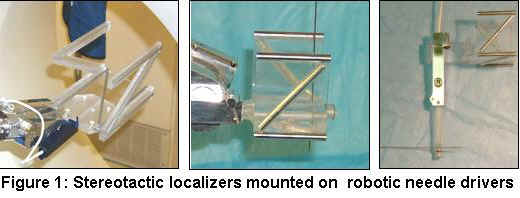
Surgical robotics has received significant publicity lately. Recent demonstrations of trans-Atlantic telesurgical gallbladder removal with the Zeus system or coronary bypass surgery on a beating heart with the daVinci system received much attention. Several robotic systems are available for commercial use in the US, yet many of their fundamental operating principles are still unknown or not studied in a through and systematic manner. One of such unexplored issues is robustness of the registration between the robot’s coordinate frame and the reference system in which the anatomical target is located. Clearly, this is one of the most critical elements in computational image-guided surgical robotic system. Failure of registration will either cause harm to the patient if remains unnoticed or it causes the surgical procedure to halt, which may cerate equally dangerous situations. Typically, we track the robot’s end-effector by the means of some imaging device. Ideally, this imaging device is the same anatomical or physiological medical imaging modality (X-ray, MRI, Ultrasound) that guides the surgical procedure, but it can be some infrared or visible light snapshot or video stream. In order to facilitate registration, we attach precision machined localizer fixtures (a.k.a fiducials) to the end-effector [1,2,3,4], as shown in Figure 1. |
 During the registration process, we extract the artifacts of the fiducials from the tracking images, then we determine the geometrical transformation between the coordinate frames of the fixture and the imager. This registration typically produces a transformation between the coordinate frame of the end-effector and the coordinate frame of the imager. The transformation implements six degrees of freedom motion in the three dimensional space, hence the historic name “stereotactic registration.” A similar concept has been used for several decades in FDA approved products for stereotactic target localization in neurosurgery and radiosurgery [5-12], as shown in Figure 2. The same concept has also emerged in research systems for extra-cranial stereotaxis [13-17]. It is conceivable, therefore, that a row of surgical robot systems will claim substantial equivalency in stereotactic registration on this basis, in the near future. During the registration process, we extract the artifacts of the fiducials from the tracking images, then we determine the geometrical transformation between the coordinate frames of the fixture and the imager. This registration typically produces a transformation between the coordinate frame of the end-effector and the coordinate frame of the imager. The transformation implements six degrees of freedom motion in the three dimensional space, hence the historic name “stereotactic registration.” A similar concept has been used for several decades in FDA approved products for stereotactic target localization in neurosurgery and radiosurgery [5-12], as shown in Figure 2. The same concept has also emerged in research systems for extra-cranial stereotaxis [13-17]. It is conceivable, therefore, that a row of surgical robot systems will claim substantial equivalency in stereotactic registration on this basis, in the near future. |
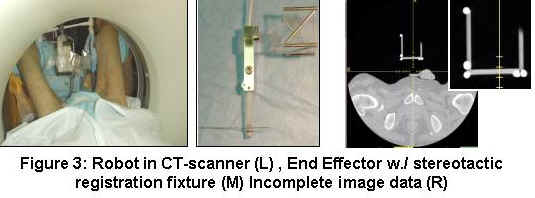 Failure to register the robot to the imager’s coordinate space may be caused by several factors. Most typically, the localizer fixture cannot be identified clearly in the images or some of its features are amiss and we lose information from the registration process. As a consequence, the accuracy of registration declines and at some point the registration may become impossible. Throughout the history of stereotactic registration, the prime directive in determining the ideal shape and size for registration fixtures has been “simplicity”, while robustness to variability of pose was not considered seriously. Currently, all FDA approved stereotactic localizer devices like the BRW, CRW, Leksell, Leibinger, Brainlab, or Elekta stereotactic localizer frames are delivered with some sort of a computer program or calculation method to perform the registration. All of these products employ three times the amount of mathematically necessary and sufficient information, yet any loss from that information causes their registration algorithm to fail. Fortunately, this situation can be prevented in conventional neurosurgery or radiosurgery procedures, where the imaging procedure is performed off-line, prior to the actual surgery. Pre-operative imaging is performed under strict protocol, when the stereotactic localizer device is not allowed to move within the field of the imager. In surgical robotics, however, we deal with a grossly different scenario, as the end-effector (with along the registration fixture) moves in the imaging field and visibility of the fixture changes constantly. As a consequence, some features can be in obstruction or parts of the fixture may move outside the field of view, as shown in Figure 3. Failure to register the robot to the imager’s coordinate space may be caused by several factors. Most typically, the localizer fixture cannot be identified clearly in the images or some of its features are amiss and we lose information from the registration process. As a consequence, the accuracy of registration declines and at some point the registration may become impossible. Throughout the history of stereotactic registration, the prime directive in determining the ideal shape and size for registration fixtures has been “simplicity”, while robustness to variability of pose was not considered seriously. Currently, all FDA approved stereotactic localizer devices like the BRW, CRW, Leksell, Leibinger, Brainlab, or Elekta stereotactic localizer frames are delivered with some sort of a computer program or calculation method to perform the registration. All of these products employ three times the amount of mathematically necessary and sufficient information, yet any loss from that information causes their registration algorithm to fail. Fortunately, this situation can be prevented in conventional neurosurgery or radiosurgery procedures, where the imaging procedure is performed off-line, prior to the actual surgery. Pre-operative imaging is performed under strict protocol, when the stereotactic localizer device is not allowed to move within the field of the imager. In surgical robotics, however, we deal with a grossly different scenario, as the end-effector (with along the registration fixture) moves in the imaging field and visibility of the fixture changes constantly. As a consequence, some features can be in obstruction or parts of the fixture may move outside the field of view, as shown in Figure 3. |
Loss of stereotactic registration information is inevitable in surgical robotic systems, yet this issue has not been researched in depth. Our group has published results of an initial investigation that revealed intriguing results and many implications to manufacturing of registration hardware and software. We also concluded that new research should be directed toward analyzing the performance of currently known systems and development of novel computational solutions and registration methods that perform robustly under sub-optimal working conditions, when only partial information is available. As robotic technology advances, end-effectors can be introduced into the body, in order to control surgical tools locally. When the end-effector is inside the body, the localizer fixture must be built inside the end-effector, in a way that it does not obstruct the actuation mechanism. This restriction calls for geometrically complex fiducial patterns, which, in turn, also require computationally intensive numerical solutions. On the other hand, novel high-performance numerical computational methods could also make sophisticated fiducial patterns technically feasible.